Table of Contents
📋 PART 1: Introduction & Preparation
Everything you need to know before starting your SHA Part A
What is SHA Part A?
The Separation Health Assessment (SHA) Part A Self-Assessment is a 16-page medical history form required by the VA for all service members filing BDD (Benefits Delivery at Discharge) or IDES claims since April 1, 2023.
✅ Why This Form Matters
- Determines Your C&P Exams: The VA uses this form to decide which C&P exams to schedule
- Establishes Your Claim: This is YOUR chance to tell your story before the VA examiner sees you
- Documents Everything: Captures conditions that might not be in your service medical records yet
- Protects Future Claims: Environmental exposures documented now = easier claims decades later
📦 What You Need to Gather BEFORE You Start
📄 Service Medical Records
- All sick call visits
- Profile documentation
- Physical therapy records
- Specialty consultations
💡 Request from your medical records office. Consider using a portable document scanner to digitize everything.
🎖️ Deployment Documentation
- Deployment orders
- DD-214 (if prior service)
- Awards and decorations
- Unit assignment history
💡 Store originals in a fireproof document safe.
💊 Medication Information
- Current prescriptions
- Over-the-counter meds
- Supplements and vitamins
- Past medications tried
💡 Call your pharmacy for a complete list.
📅 Timeline & Dates
- When symptoms started
- Injury incident dates
- Surgery dates
- Deployment timeframes
💡 Approximations are okay (month/year).
🎯 The WHEN-WHAT-HOW-NOW Format
Throughout this guide, you’ll document every condition using this proven 4-part format:
Documentation Template
When It Started
Date/timeframe symptoms began. Connect to deployment, training, or incident.
Example: “Started during Iraq deployment, March 2019”
What Your Symptoms Are
Detailed description of what you feel/experience. Be specific.
Example: “Constant high-pitched ringing in both ears, 24/7, loudness 6/10”
How It Affects You
Functional limitations. What can’t you do? Impact on work, family, life.
Example: “Can’t sleep without white noise, difficulty concentrating at work”
Current Status
Present situation, treatments, medications, prognosis.
Example: “Permanent condition per audiologist, using white noise machine nightly”
💡 Pro Tip: This format works for EVERY condition – physical or mental health. Master it now and you’ll breeze through the entire form.
📊 Top 50 Most Claimed VA Disabilities (We Cover All of Them)
| Rank | Condition | Category | Where Covered in Guide |
|---|---|---|---|
| #1 | Tinnitus | Hearing | Part 5 |
| #2 | Knee Limitation of Flexion | Musculoskeletal | Part 4 |
| #3 | Sciatica (Paralysis of Sciatic Nerve) | Back/Spine | Part 4 |
| #4 | Lumbosacral/Cervical Strain | Back/Neck | Part 4 |
| #5 | Hearing Loss | Hearing | Part 5 |
| #6 | PTSD | Mental Health | Part 3 |
| #7 | Shoulder Limitation of Motion | Musculoskeletal | Part 4 |
| #8 | Ankle Limitation of Range of Motion | Musculoskeletal | Part 4 |
| #9-50 | Plus 42 more conditions covered throughout this guide… | ||
View detailed guides for top conditions:
⏰ Timeline: When to Complete This Form
BDD Filing Timeline
- 90-180 days before separation: You MUST file within this window
- Earlier is better: Gives you time to gather evidence, get buddy statements
- Allow 6-8 hours: To complete this form thoroughly (do NOT rush!)
- Break it into sessions: Complete 1-2 sections per sitting
🚀 Ready to Begin?
You’ve Got This! 💪
Thousands of service members have used this guide to maximize their VA ratings. You’re about to document your service-connected conditions like a pro.
Estimated Time: 6-8 hours total (break into sessions)
What You’ll Learn: How to document 50+ conditions with VA keywords and functional limitations
Start Part 2: Section I →📋 PART 2: Section I (Identification) & Section II Questions 1-21
Basic personal/military info and initial medical history questions
Section I: Identification Information
This is the easy part – basic identifying information. Fill this out like any military form you’ve completed before.
What You’ll Need:
- Personal Info: Full name, SSN, date of birth, current address
- Contact Info: Phone numbers (work and personal), email addresses (military and civilian)
- Military Info: Branch, rank, MOS/rate, unit, duty station
- Separation Info: ETS/separation date, type of claim (BDD, IDES, Standard)
💡 Contact Information is CRITICAL: Use your civilian email as primary contact. Your .mil email will be deleted 30-90 days after separation. The VA will use this contact info to schedule your C&P exams.
Section II: Report of Medical History – Initial Questions
Question 1: Current Medications
List EVERYTHING you’re currently taking:
- Prescription medications (name, dose, frequency, what it’s for)
- Over-the-counter medications (if taken regularly)
- Supplements and vitamins
- Pain relievers taken regularly (even ibuprofen counts!)
Example Medication List:
- Sertraline 100mg, daily (for PTSD/depression) - Trazodone 50mg, nightly (for insomnia) - Meloxicam 15mg, daily (for knee and back pain) - Ibuprofen 800mg, as needed 3-4x/week (for pain) - Vitamin D 2000 IU, daily
Questions 2-5: Overall Health Assessment
Answer honestly about your current health status. The VA wants to know:
- Has your health gotten worse since your last physical?
- Do physical health problems make it hard to do your job?
- Do you need special equipment (CPAP, hearing aids, orthotics)?
⚠️ Don’t Downplay: If you’re taking ibuprofen daily, your back hurts after standing for 2 hours, or you can’t run without knee pain – SAY SO. The VA needs to know how conditions affect your daily function.
Questions 6-21: Specific Medical Conditions
These questions ask about major medical conditions. For each YES answer, use the WHEN-WHAT-HOW-NOW format.
Heart/Cardiovascular
High blood pressure, heart disease, chest pain
Respiratory
Asthma, COPD, chronic cough, sleep apnea
Digestive
GERD, IBS, chronic stomach problems
Endocrine
Diabetes, thyroid problems, metabolic issues
Continue to Part 3 for mental health conditions (PTSD, depression, TBI, migraines)…
Part 3: Mental Health & Cognitive Conditions (Questions 22-35)
Understanding Mental Health Claims
Mental health conditions are among the most common and most challenging VA disability claims. The SHA Part A form dedicates 14 questions (22-35) to mental health screening because:
- High prevalence: Over 1.5 million veterans receive compensation for mental health conditions
- Complex documentation: Requires linking symptoms to specific service events/stressors
- Multiple manifestations: Same trauma can cause PTSD, depression, anxiety, sleep disorders
- Secondary conditions: Mental health issues often cause physical problems (migraines, IBS, hypertension)
Top Mental Health Conditions by Claim Volume
| Condition | Ranking | Symptoms to Document | Common Rating |
|---|---|---|---|
| PTSD | #6 | Flashbacks, nightmares, hypervigilance, avoidance, mood changes | 50-70% |
| TBI | #14 | Memory loss, headaches, dizziness, concentration issues, irritability | 0-100% |
| Depression | #23 | Persistent sadness, loss of interest, sleep changes, suicidal thoughts | 30-70% |
| Anxiety | #28 | Excessive worry, panic attacks, physical tension, social withdrawal | 30-50% |
| Sleep Disorders | #11 | Insomnia, sleep apnea, nightmares, restless sleep | 0-100% |
The WHEN-WHAT-HOW-NOW Format for Mental Health
- WHEN: Specific incidents, deployments, training events, dates
- WHAT: Detailed symptoms (frequency, intensity, duration)
- HOW: Functional impairment (work, relationships, daily activities)
- NOW: Current treatment, medications, hospitalizations
Question 22-23: PTSD & Combat Trauma
Condition: Post-Traumatic Stress Disorder (Combat-Related)
WHEN: Symptoms began during deployment to Afghanistan, September 2011 – April 2012. Specific incident: October 15, 2011 – IED strike on convoy killed two soldiers in vehicle ahead of mine. Multiple firefights during patrol operations in Kandahar Province.
WHAT: Daily symptoms include:
- Intrusive memories and flashbacks (4-5 times per week)
- Nightmares about combat (5-6 nights per week)
- Hypervigilance in public spaces (constant scanning for threats)
- Exaggerated startle response to loud noises
- Avoidance of crowds, Fourth of July fireworks, war movies
- Emotional numbness, detachment from family
- Irritability and angry outbursts (2-3 times per week)
- Difficulty concentrating on tasks for more than 10-15 minutes
HOW: Functional limitations:
- Work: Can’t attend company meetings (crowds trigger anxiety), called out sick 8 days last month due to nightmares/lack of sleep
- Relationships: Divorced in 2018 (spouse cited emotional distance, angry outbursts), limited contact with 2 children
- Social: Stopped attending church, avoid shopping malls, grocery shop at 6am to avoid crowds
- Sleep: Average 3-4 hours per night, wake in cold sweats from nightmares
NOW: Currently receiving treatment at VA Mental Health Clinic since June 2020:
- Weekly therapy sessions with Dr. Sarah Johnson, Psychologist
- Medications: Prazosin 2mg for nightmares, Sertraline 100mg for PTSD
- Participated in Cognitive Processing Therapy (12 sessions, 2021)
- One psychiatric hospitalization (March 2019, 5 days, suicidal ideation)
Supporting Documentation:
- VA mental health treatment records (2020-present)
- Deployment orders and DD-214 showing combat deployment
- Buddy statements from 3 soldiers who witnessed IED attack
- Medication list from VA pharmacy
Condition: PTSD from Military Sexual Trauma
WHEN: Sexual assault occurred during Basic Training at Fort Leonard Wood, Missouri in August 2015. Incident involved senior drill sergeant. Reported to command in September 2015, transferred to different unit.
WHAT: Symptoms that began immediately after assault and persist today:
- Intrusive memories of the assault (daily)
- Panic attacks when around authority figures (2-3 per week)
- Avoidance of men who resemble perpetrator
- Nightmares about the assault (4-5 nights per week)
- Severe anxiety in closed spaces or when alone with male colleagues
- Depression, feelings of shame and guilt
- Self-harm behaviors (cutting, controlled with therapy)
HOW: Daily life impact:
- Work: Requested transfer to all-female work section, can’t work alone with male supervisors
- Relationships: Unable to maintain intimate relationships, trust issues with men
- Physical: Developed irritable bowel syndrome (stress-related), chronic migraines
- Safety: Triple-lock all doors, sleep with lights on, keep pepper spray at bedside
NOW: In active treatment since 2016:
- Weekly therapy with MST coordinator at VA
- Medications: Zoloft 150mg, Prazosin 4mg, Xanax 0.5mg PRN
- Completed Prolonged Exposure Therapy (15 sessions)
- Attending women veterans support group (monthly)
Supporting Documentation:
- VA MST treatment records
- Restricted Report from 2015 (SAPR documentation)
- Transfer orders showing unit change
- Buddy statement from roommate who witnessed emotional aftermath
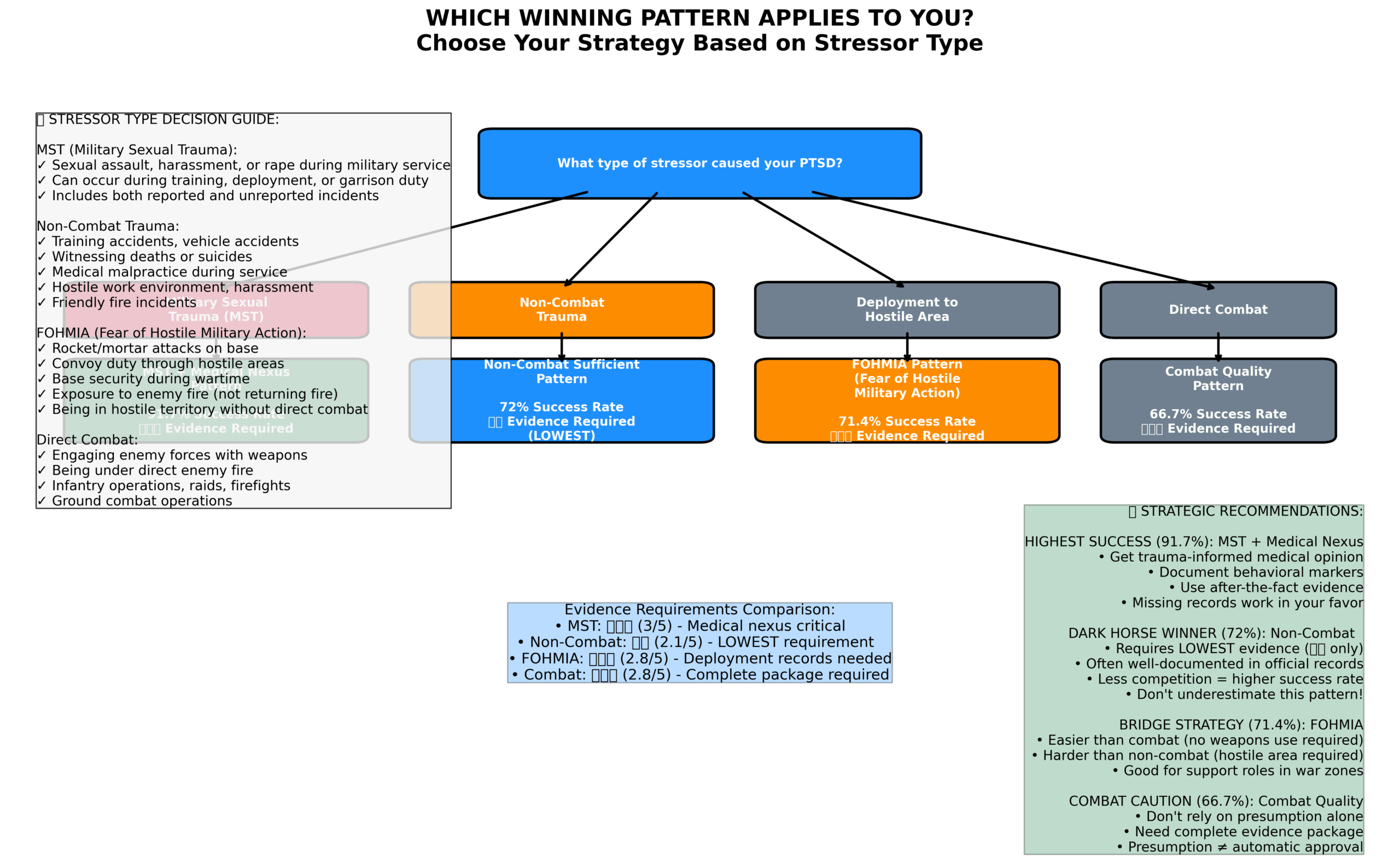
- Combat PTSD: Deployment orders, awards (CAB, CIB), unit histories suffice – don’t need to prove every firefight
- MST PTSD: Don’t need proof assault occurred – behavior changes, buddy statements, transfer requests support claim
- Non-combat PTSD: Training accidents, vehicle accidents, witnessing death – document the event and your symptoms
- VA recognizes: You don’t need an official report or criminal investigation for MST claims
Question 24-26: Depression & Mood Disorders
Condition: Major Depressive Disorder (Service-Connected)
WHEN: Depression symptoms began during deployment to Iraq (2008-2009). Worsened significantly after witnessing multiple casualties during mortar attacks on FOB. Continued after separation in 2012.
WHAT: Daily symptoms include:
- Persistent sadness and emptiness (most days)
- Loss of interest in activities I used to enjoy (fishing, sports, time with kids)
- Fatigue and low energy (struggle to get out of bed)
- Difficulty concentrating (can’t read more than a page, forget conversations)
- Feelings of worthlessness and guilt (survivor’s guilt from deployment)
- Changes in appetite (lost 30 lbs in 6 months)
- Suicidal thoughts (passive – wish I hadn’t survived, no active plan)
HOW: Functional limitations:
- Work: Lost job in 2020 due to absenteeism (missed 40+ days), currently unemployed
- Self-care: Shower 2-3 times per week, wear same clothes for days, skip meals
- Social: Isolated from friends and family, don’t answer phone calls, haven’t left house in 3 weeks except for VA appointments
- Parenting: Ex-spouse has primary custody, struggle to engage with children during visitation
NOW: In treatment since 2013:
- Monthly psychiatrist appointments with Dr. Michael Chen, VA
- Medications: Effexor XR 225mg, Wellbutrin 300mg, Trazodone 100mg for sleep
- Two psychiatric hospitalizations (2019: 7 days, 2022: 14 days) for suicidal ideation
- Participated in intensive outpatient program (6 weeks, 2022)
Question 27-28: Anxiety Disorders
Condition: Generalized Anxiety Disorder with Panic Disorder
WHEN: Anxiety symptoms began during active duty (2014-2018) due to high-stress job in military intelligence. Frequent panic attacks started during deployment to South Korea in 2016.
WHAT: Symptoms occur daily:
- Excessive worry about multiple things (work, health, finances, family safety) – 6+ hours per day
- Physical tension (jaw clenching, muscle tightness in neck/shoulders)
- Restlessness and feeling “on edge” constantly
- Difficulty concentrating due to racing thoughts
- Panic attacks 3-4 times per week: sudden intense fear, heart racing (up to 140 bpm), sweating, trembling, shortness of breath, feeling of dying
- Anticipatory anxiety about having panic attacks in public
HOW: Daily impact:
- Work: Avoid presentations, conference calls, team meetings due to fear of panic attack
- Driving: Can’t drive on highways (panic attacks in traffic), limited to local roads, plan routes with multiple exits
- Social: Decline social invitations, avoid restaurants/movies, fear of being trapped
- Physical: ER visits 6 times in past year thinking having heart attack (all anxiety-related)
NOW: Treatment since 2017:
- Bi-weekly therapy with psychologist, CBT for anxiety management
- Medications: Lexapro 20mg daily, Ativan 1mg PRN (use 4-5 times/week)
- Tried multiple medications (Prozac, Zoloft, Paxil) with limited success
Question 29-31: Traumatic Brain Injury (TBI)
Condition: Traumatic Brain Injury (Mild) with Post-Concussive Syndrome
WHEN: Initial injury: March 2012, IED blast in Afghanistan. Lost consciousness for approximately 2 minutes, dazed and confused for 30+ minutes after. Medic evaluation at FOB noted probable concussion. Returned to duty after 48 hours. Second blast exposure: June 2012, no loss of consciousness but saw “stars” and had severe headache. Third exposure: August 2012, vehicle rollover, hit head on roof.
WHAT: Persistent symptoms since 2012:
- Cognitive: Memory problems (forget appointments, conversations, where I put things), difficulty concentrating (can’t read for more than 10 minutes), mental fog, slow information processing
- Headaches: Daily headaches (6/10 severity), worsen with noise, light, stress, occur behind eyes and temples
- Dizziness: Balance problems, vertigo when standing quickly, feel unsteady 3-4 times per week
- Sensory: Light sensitivity (wear sunglasses indoors), noise sensitivity (need quiet environment), ringing in ears
- Sleep: Insomnia, difficulty falling asleep, frequent waking
- Mood: Irritability, quick to anger, emotional lability (cry easily)
HOW: Functional limitations:
- Work: Can’t work in open office (noise/light triggers), need written instructions (can’t remember verbal), work from home 4 days/week
- Driving: Lost license for 3 months in 2019 due to episodes of confusion while driving, still avoid driving at night or in heavy traffic
- Daily tasks: Use phone calendar for everything, sticky notes throughout house, wife manages all finances/appointments
- Social: Can’t attend concerts, sporting events, loud restaurants – trigger severe headaches and dizziness
NOW: Ongoing treatment since 2013:
- Enrolled in VA TBI clinic, seen by neurologist every 3 months
- Cognitive rehabilitation therapy (completed 20 sessions in 2020)
- Vestibular therapy for balance issues (ongoing)
- Medications: Topiramate 100mg for headaches, Amitriptyline 50mg at bedtime
- MRI (2019): showed no acute findings but documented history of TBI
- Neuropsych evaluation (2021): documented cognitive impairment in memory and processing speed
Supporting Documentation:
- Combat medic notes from 2012 (if available)
- VA TBI screening results and treatment records
- Neuropsychological evaluation report
- MRI results
- Buddy statements describing personality changes and cognitive issues
- Don’t need: Proof of initial concussion diagnosis (many TBIs went undiagnosed during deployment)
- Do need: Credible evidence of injury during service (blast exposure, vehicle accident, fall, etc.)
- Key evidence: Current persistent symptoms + exposure event + medical nexus
- Buddy statements crucial: Friends/family describing cognitive changes, personality changes since service
- Neuropsych testing: Objective evidence of cognitive impairment strengthens claim significantly
Question 32-33: Sleep Disorders
Condition: Obstructive Sleep Apnea (claiming secondary to PTSD and obesity from medications)
WHEN: Sleep problems began with PTSD (service-connected at 70% since 2016). Diagnosed with sleep apnea in 2019 after VA sleep study. Weight gain (60 lbs) attributed to PTSD medications (Mirtazapine, Seroquel).
WHAT: Sleep symptoms include:
- Stop breathing during sleep (witnessed by spouse 10+ times per night)
- Loud snoring every night
- Gasping or choking during sleep
- Excessive daytime sleepiness (fall asleep during conversations, while driving)
- Morning headaches (daily)
- Difficulty concentrating during day due to fatigue
- Irritability from poor sleep quality
HOW: Functional impact:
- Work: Called to HR 3 times for sleeping at desk, nearly fired
- Driving: Minor accident in 2021 (fell asleep at red light, rear-ended car ahead)
- Relationships: Sleep in separate bedroom from spouse (snoring too loud)
- Health: Developed high blood pressure (started 2020, likely related to sleep apnea)
NOW: Current treatment:
- CPAP machine prescribed January 2020 (ResMed AirSense 10)
- CPAP compliance: use 6-7 nights per week, 7+ hours per night
- CPAP data shows AHI reduced from 42 to 3.5 with treatment
- Still experiencing daytime fatigue despite CPAP use
- Follow-up sleep studies (2021, 2023) confirm ongoing apnea
Nexus to Service-Connected Conditions:
- PTSD medications (Mirtazapine 45mg, Seroquel 300mg) both list weight gain as side effect
- Gained 60 lbs since starting medications in 2017 (175 lbs to 235 lbs)
- Sleep disturbance from PTSD nightmares contributes to sleep apnea severity
- Request VA Independent Medical Opinion (IMO) or private nexus letter linking sleep apnea to service-connected PTSD
Question 34-35: Cognitive & Memory Issues
Condition: Cognitive Impairment secondary to TBI and PTSD
WHEN: Cognitive problems began after TBI in 2013 (blast exposure in Afghanistan) and worsened with development of PTSD. Both conditions now service-connected (TBI at 10%, PTSD at 50%).
WHAT: Cognitive symptoms include:
- Memory: Short-term memory severely impaired (forget conversations within minutes, can’t remember if I took medication, lose items constantly)
- Concentration: Can’t focus on single task for more than 5-10 minutes, easily distracted
- Processing speed: Takes me much longer to understand instructions, need information repeated multiple times
- Executive function: Difficulty planning, organizing, making decisions (paralyzed by simple choices)
- Word-finding: Struggle to find the right words, lose train of thought mid-sentence
HOW: Daily limitations:
- Work: Went from complex IT work to simple data entry, still make frequent errors, received performance improvement plan
- Daily living: Rely on wife for all planning, scheduling, finances, household management
- Safety: Left stove on 4 times (smoke detector saved house twice), wife hides car keys at night
- Independence: Can’t live independently, need supervision for medication, appointments, daily tasks
NOW: Ongoing treatment and documentation:
- Neuropsychological evaluation (2022): documented deficits in memory, processing speed, executive function (scores 2+ standard deviations below age-matched peers)
- Cognitive rehabilitation therapy (ongoing, limited improvement)
- Occupational therapy to develop compensatory strategies
- Use of memory aids: phone alarms, written lists, pill organizer, GPS for navigation
Requesting Increase: Filing for increase of TBI rating based on cognitive symptoms. Current neuropsych testing supports higher rating.
Mental Health Documentation Strategy
1. Establish the In-Service Stressor/Event:
- Combat: deployment orders, awards, unit history
- MST: behavior changes, buddy statements, transfer requests
- Accident/injury: incident reports, medical records, witness statements
- TBI: blast exposure, vehicle accidents, head injuries
2. Document Current Symptoms (Detailed!):
- Frequency: how often symptoms occur (daily, weekly)
- Intensity: severity on 1-10 scale, impact on functioning
- Duration: how long symptoms last
- Triggers: what makes symptoms worse
3. Show Functional Impairment:
- Work: missed days, performance issues, accommodations needed, job loss
- Relationships: divorces, estrangement, conflicts
- Social: isolation, avoidance, inability to maintain friendships
- Self-care: hygiene, nutrition, sleep, daily routines
4. Evidence of Ongoing Treatment:
- Therapy: frequency, type (CBT, CPT, PE), provider names
- Medications: names, doses, side effects, effectiveness
- Hospitalizations: dates, reasons, length of stay
- Treatment compliance: show you’re actively seeking help
5. Buddy Statements are CRITICAL:
- Spouse/family describing personality changes, behavioral changes
- Fellow service members who witnessed stressor events
- Friends who can compare pre-military vs. post-military behavior
- Coworkers describing work performance decline
Common Mental Health Rating Levels
| Rating | Key Symptoms Required | Functional Impact |
|---|---|---|
| 0% | Diagnosed condition, minimal symptoms | No occupational or social impairment |
| 10% | Mild symptoms during high stress | Slight occupational/social impairment |
| 30% | Occasional decrease in work efficiency, mild symptoms | Some difficulty in social/work situations |
| 50% | Reduced reliability, difficulty maintaining relationships | Moderate occupational and social impairment |
| 70% | Severe symptoms affecting most areas of life | Severe occupational/social impairment, suicidal ideation |
| 100% | Total impairment in all areas | Inability to function independently, persistent danger |
- Be honest about bad days: Don’t just describe average days – tell examiner about your worst days
- Bring symptom log: Track symptoms for 30 days before exam (frequency, intensity, impact)
- Describe functional impact: How symptoms affect work, relationships, self-care, social activities
- Mention hospitalizations: Psychiatric hospitalizations are strong evidence of severity
- List all medications: Multiple medications or high doses indicate severity
- Discuss suicidal thoughts: If you’ve had them (past or present), tell the examiner
- Bring someone with you: Spouse/family member can provide observations and support
- Don’t minimize: Veterans often downplay symptoms – be detailed and honest
Secondary Conditions to Consider
Mental health conditions often cause or worsen other conditions. Consider filing secondary claims for:
| Primary Condition | Common Secondary Conditions | Nexus Explanation |
|---|---|---|
| PTSD | Sleep apnea, IBS, migraines, erectile dysfunction, hypertension | PTSD medications cause weight gain → sleep apnea; chronic stress → physical conditions |
| TBI | Migraines, sleep disorders, cognitive dysfunction, depression | Brain injury directly causes headaches, sleep problems, mood changes |
| Depression | Obesity, sleep disorders, chronic pain | Depression reduces activity → weight gain; disrupts sleep; lowers pain tolerance |
| Anxiety | IBS, GERD, hypertension, panic disorder | Chronic anxiety causes GI issues, raises blood pressure, triggers panic attacks |
Mental Health Resources
- PTSD Appeal Strategy: Complete PTSD BVA Appeal Guide
- TBI Appeal Strategy: TBI BVA Appeal Guide
- Migraine Appeal Strategy: Migraine BVA Appeal Guide
- VA Crisis Line: Call 988, then press 1 (24/7 support for veterans in crisis)
- Veterans Crisis Line: Text 838255 (confidential text support)
- VA Mental Health Portal: www.mentalhealth.va.gov
- Vet Centers: Free counseling for combat veterans and MST survivors (no VA enrollment required)
For comprehensive PTSD guidance, consider The Veteran’s PTSD Handbook – written by veterans, for veterans. Covers symptoms, treatments, VA claims process, and coping strategies. (~$15-20)
Critical Reminders for Mental Health Claims
- ✅ Stressor event documented: When, where, what happened (specific dates/details)
- ✅ Symptoms detailed: All symptoms with frequency, intensity, duration, triggers
- ✅ Functional impairment shown: How symptoms affect work, relationships, daily life
- ✅ Treatment documented: All providers, medications, therapies, hospitalizations
- ✅ Buddy statements obtained: At least 2-3 statements from people who’ve witnessed changes
- ✅ Secondary conditions considered: File for related physical conditions
- ✅ Symptom log prepared: 30-day tracking before C&P exam
- ✅ Honesty committed: Will describe worst days, not minimize symptoms at exam
Remember: Mental health claims have high approval rates when properly documented. The VA expects mental health issues from combat exposure, MST, and traumatic service events. Don’t minimize your symptoms or feel shame about seeking help. These are legitimate medical conditions caused by your service to our nation.
Next Section: Now that we’ve covered mental health (Questions 22-35), let’s move on to Part 4 where we’ll document musculoskeletal conditions – back pain, joint problems, and physical injuries that affect your daily functioning.
🦴 PART 4: Musculoskeletal System (Joints, Spine & Body Regions)
Back pain, knee injuries, shoulder problems, and all joint/muscle conditions
Why This Section is HUGE for VA Claims
Military service is HARD on the body. This section covers some of the most commonly claimed conditions:
- #2 Knee Limitation of Flexion
- #3 Sciatica (pain down leg)
- #4 Back Pain (lumbosacral/cervical strain)
- #7 Shoulder Limitation of Motion
- #8 Ankle Problems
- Plus: Hip pain, wrist/hand issues, foot problems (#19 Flat Feet, #26 Plantar Fasciitis)
📖 Detailed Condition Guides:
- Back & Spine Appeals Guide – Maximize your back pain rating
- Knee Appeals Guide – Knee condition documentation strategies
- Shoulder Appeals Guide – Shoulder limitation of motion
8 Body Regions to Document
The form asks about pain/problems in these regions. For each YES answer, provide detailed documentation:
1️⃣ Head and Neck
Neck pain, cervical strain, limited neck movement, TMJ
2️⃣ Back and Chest
Low back pain, sciatica, thoracic pain, rib injuries
3️⃣ Shoulder and Arm
Rotator cuff, limited range of motion, weakness, surgery
4️⃣ Elbow and Forearm
Tennis elbow, limited motion, pain with gripping
5️⃣ Wrist, Hand, Fingers
Carpal tunnel (#30), trigger finger, arthritis
6️⃣ Hip and Thigh
Hip pain, bursitis, limited motion, IT band issues
7️⃣ Leg and Knee
Knee pain, meniscus tears, instability, swelling
8️⃣ Ankle, Foot, Toes
Plantar fasciitis, flat feet, ankle sprains
📝 Example: Back Pain with Sciatica (#3 & #4 Most Claimed)
Documenting Lower Back Pain and Sciatica
🗓️ WHEN: “Started during 2018 Iraq deployment. Noticed pain after long ruck marches and vehicle patrols. Got worse over time. First reported to TMC October 2018.”
📋 WHAT: “Constant dull ache in lower back (lumbar region). Sharp stabbing pain with bending or lifting. Pain RADIATES DOWN LEFT LEG (sciatica) – shooting pain from low back through left buttock, down back of left thigh, sometimes to left foot. Left leg has numbness and tingling, especially foot and toes.”
⚠️ HOW: “Can’t complete full ruck marches – pain becomes unbearable (7-8 out of 10). Can’t sit for more than 45 minutes without needing to stand. Can’t lift objects over 40 lbs. Sleep affected – need pillow between knees. Can’t play with kids without pain.”
✅ NOW: “Daily pain 4-6 out of 10, worse with activity. Completed physical therapy (2 rounds). Take Meloxicam daily. Had MRI showing disc bulges. On permanent profile (no running, limited lifting). Pain is NOT improving despite treatment.”
🔥 CRITICAL: Sciatica vs. Back Pain
If you have LOW BACK PAIN that shoots down your LEG = SCIATICA (#3 most claimed).
Mention the leg pain separately! Sciatica can be rated separately from back pain, potentially doubling your rating.
Keywords VA looks for: “radiating pain down leg,” “shooting pain into buttock/leg,” “numbness/tingling in leg or foot”
📝 Example: Knee Pain (#2 Most Claimed)
Bilateral Knee Pain with Limitation of Flexion
🗓️ WHEN: “Started during Iraq deployment 2018-2019. Gradual onset from running, rucking, and patrols. Both knees affected, right worse. First TMC visit December 2018.”
📋 WHAT: “Constant aching in both knees. Sharp pain going down stairs. Stiffness after sitting. Both knees swell after activity. Grinding/crunching sensation when squatting (crepitus). Can’t fully bend right knee.”
⚠️ HOW: “Can’t complete PT runs – pain forces me to stop. Can’t ruck with full load. Going downstairs is painful – have to go sideways. Can’t kneel (affects work tasks). Can’t squat fully. Affects playing with kids.”
✅ NOW: “Daily pain 5-7/10, worse with stairs. X-rays show early arthritis. Completed physical therapy (10 sessions). Wear knee sleeves daily. On permanent profile (no running, no jumping). Considering cortisone injection.”
💡 Pro Tips for Knee Documentation:
- Describe INSTABILITY (“knee gives out,” “feels like it will buckle”)
- Note SWELLING (when does it swell? after what activities?)
- Mention CLICKING/POPPING/GRINDING sounds
- Describe STAIR difficulties (up vs. down)
- Include KNEELING limitations (important for military tasks)
- Note if you can’t fully BEND or STRAIGHTEN knee
Quick Reference: Other Common Musculoskeletal Conditions
| Condition | Key Symptoms to Document | VA Keywords |
|---|---|---|
| Shoulder Problems | Can’t lift arm overhead, can’t reach behind back, clicking/popping, weakness | “Limitation of motion,” “painful arc,” “rotator cuff” |
| Flat Feet (#19) | Arch pain, ankle rolling inward, causes knee/back pain, need orthotics | “Pes planus,” “pronation,” “symptomatic” |
| Plantar Fasciitis (#26) | Heel pain, WORST with first steps in morning, “stepping on glass” feeling | “Plantar fasciitis,” “morning pain,” “heel pain” |
| Carpal Tunnel (#30) | Hand numbness/tingling (especially thumb/index/middle fingers), worse at night, wake up with numb hands | “Carpal tunnel syndrome,” “median nerve,” “nighttime symptoms” |
Need Help with Musculoskeletal Claims?
Use our VA Disability Calculator to estimate your combined rating with multiple joint conditions.
👂 PART 5: Hearing, Vision, TBI & Environmental Exposures
Tinnitus (#1!), hearing loss, vision problems, burn pits, and hazardous exposures
🔔 Tinnitus – THE #1 MOST CLAIMED VA DISABILITY
2.9+ million veterans have service-connected tinnitus. If you hear ANY ringing, buzzing, or hissing in your ears – REPORT IT.
Documenting Tinnitus (Use This Template!)
🗓️ WHEN: “Started during Iraq deployment 2018. Noticed after firefight in July 2018. Got worse after IED explosion April 2018. Became constant by end of deployment.”
📋 WHAT: “Constant high-pitched ringing in both ears, sounds like ‘eeeeeee’. Present 24/7 – NEVER goes away. Louder in right ear. Gets louder in quiet environments. Volume usually 5-6 out of 10.”
⚠️ HOW: “Difficulty falling asleep – need white noise machine. Can’t concentrate in quiet environments – ringing is distracting. Difficulty hearing conversations in noisy places (restaurant, crowds). Extremely annoying and frustrating. Sometimes causes headaches.”
✅ NOW: “Tinnitus is constant, permanent, 24/7. Had audiology evaluation confirming tinnitus. Audiologist said no cure. Use white noise machine every night. Trying to habituate but very difficult.”
🎯 CRITICAL: List ALL Noise Exposures!
This is HOW you prove service connection for tinnitus and hearing loss:
🔫 Weapons Fire
- M4 rifle (thousands of rounds)
- M249 SAW
- .50 cal machine gun
- Grenade launchers
- Hand grenades
💥 Explosions
- IED exposures (distances)
- Demolitions training
- Artillery simulators
- Breaching charges
✈️ Aircraft Noise
- Helicopter flights (types, frequency)
- Jet aircraft
- Flight deck operations
- Medevac helicopters
🚙 Vehicles & Equipment
- HMMWVs, MRAPs, tanks
- Generators (daily exposure)
- Heavy equipment
- Ship engine rooms
⚠️ About Hearing Protection: Even if you wore earplugs, cumulative noise exposure causes damage. In combat, hearing protection often couldn’t be worn (needed to hear threats/communications). MENTION THIS.
🔥 Burn Pit Exposure (PACT Act – CRITICAL!)
If you deployed to Iraq, Afghanistan, or other locations with burn pits – DOCUMENT THIS NOW even if you don’t have symptoms yet.
🚨 WHY THIS IS CRITICAL
The PACT Act (2022) presumes many conditions are related to burn pit exposure. Documenting exposure NOW protects future claims for:
- Respiratory conditions (asthma, bronchitis, COPD)
- Cancers
- Many other conditions
This could affect claims decades from now. Document exposure even without current symptoms!
Burn Pit Exposure Documentation
“YES, I was exposed to burn pits during deployment:
Deployment 1: Iraq, 2018-2019 (12 months)
- Location: FOB near Baghdad
- Burn pit operated 24/7, approximately 400 meters from living quarters
- Smoke and smell constant, especially at night
- Breathed smoke daily for 12 months
- Health effects: Chronic cough started during deployment, persists today
🔗 Enrolled in VA Burn Pit Registry: [Date] – Confirmation number: [if available]”
💡 ENROLL IN THE BURN PIT REGISTRY NOW:
It’s free, takes 10 minutes, and strengthens future claims.
Other Environmental/Occupational Exposures to Document
- Chemical exposures: Diesel fuel, JP-8 jet fuel, hydraulic fluids, solvents, pesticides
- Particulate matter: Desert sand/dust, “Iraq crud”
- Heavy metals: Lead (from firing ranges), depleted uranium
- Asbestos: Older ships/buildings
- Contaminated water: Camp Lejeune (if stationed there 1953-1987)
Document EVERYTHING. You can’t claim what you don’t report.
🦷 PART 6: Dental, Women’s Health & Mental Health Screening
TMJ, dental injuries, women’s health issues, and final screening questionnaires
Dental Health (TMJ #39 Most Claimed)
TMJ/TMD (temporomandibular joint disorder) is ratable, especially if secondary to PTSD (teeth grinding from stress).
TMJ Documentation
🗓️ WHEN: “Started during 2019 deployment. Began clenching jaw and grinding teeth at night from stress.”
📋 WHAT: “Jaw pain (both sides, worse on right). Jaw clicks and pops. Can’t open mouth fully (can’t fit three fingers). Frequent headaches starting at temples.”
⚠️ HOW: “Can’t eat certain foods (steak, bagels). Headaches 3-4 times per week. Difficulty during dental appointments. Affects sleep – wake up with jaw pain.”
✅ NOW: “Daily jaw pain and clicking. Dentist diagnosed TMJ. Wear night guard every night. Physical therapy for TMJ. Related to PTSD (stress-induced grinding).”
💡 TMJ Secondary to PTSD: If you grind your teeth due to PTSD, anxiety, or deployment stress – MAKE THAT CONNECTION. Secondary service connection can significantly increase your rating.
Women’s Health (For Female Service Members)
Document reproductive health issues that started or worsened during service:
- Endometriosis
- PCOS (polycystic ovary syndrome)
- Painful/irregular periods
- Pregnancy complications during service
- MST (Military Sexual Trauma) – You DON’T need an official report to claim
MST Resources:
- VA MST Coordinators at every VA Medical Center
- Confidential support: VA MST Program
- Presumptive service connection for mental health conditions
Mental Health Screening Questionnaires
The form includes short screening tools. Answer honestly – positive screens lead to appropriate evaluations.
PTSD Screening (PC-PTSD-5)
5 yes/no questions about trauma symptoms. Answering YES to 3+ = positive screen for PTSD.
Depression Screening (PHQ-2)
2 questions about interest/pleasure and feeling down. Used to identify depression.
Alcohol Use Screening (AUDIT-C)
Questions about alcohol consumption. If you’re drinking to cope with PTSD/deployment stress – SAY SO. Alcohol use disorder secondary to PTSD is a valid claim.
⚠️ Be Honest: These screenings help ensure you get proper evaluations and care. Don’t downplay symptoms to avoid “making a fuss.” Positive screens = appropriate C&P exams = accurate ratings.
📄 PART 7: Complete Example – Filled Out SHA Part A
See exactly what a thoroughly documented form looks like
Meet SSG Michael Rodriguez (Fictional Example)
Service Member Profile
- Branch: US Army
- Rank: SSG (E-6)
- MOS: 11B Infantry
- Time in Service: 8 years
Deployments
- Iraq: 2018-2019 (12 months)
- Afghanistan: 2021-2022 (9 months)
- Combat deployments with multiple exposures
Top Conditions
- PTSD (combat)
- Chronic back pain + sciatica
- Bilateral knee pain
- Right shoulder injury
Plus 11 More Conditions
- Tinnitus + hearing loss
- TBI with persistent symptoms
- Sleep apnea with CPAP
- Migraines, plantar fasciitis, more
Example: How SSG Rodriguez Documented His PTSD
WHEN did it start?
“During and after first deployment to Iraq, 2018-2019. Symptoms started during deployment but got much worse after returning home in January 2019. Officially diagnosed by Behavioral Health in June 2019.”
WHAT are your stressor events?
- PRIMARY STRESSOR: IED Explosion, April 15, 2018, Anbar Province. IED detonated near patrol. Two squad members seriously injured. Thought I was going to die.
- SECONDARY STRESSOR: Firefight, July 2018. Ambushed during patrol. Heavy enemy fire for 15 minutes. First time seeing dead bodies.
- ADDITIONAL: Multiple IED close calls, rocket attacks on FOB, death of friend (SPC Johnson)
WHAT are your current symptoms?
- Nightmares: 4-5 times per week about deployment, IED explosions. Wake up sweating, heart pounding.
- Flashbacks: Triggered by loud noises (car backfires, fireworks), helicopters, smell of diesel.
- Avoidance: Avoid crowded places, fireworks, news about Middle East, talking about deployment.
- Hypervigilance: Constantly scanning for threats, check locks multiple times, sit with back to wall, easily startled.
- Negative mood: Survivor guilt, blame myself, emotionally numb, detached from wife and kids.
- Sleep problems: Difficulty falling asleep, frequent waking, average 4-5 hours per night.
HOW does it affect your life?
- Work: Difficulty concentrating, irritability affects relationships with subordinates, career progression affected.
- Relationships: Marriage strained, don’t connect emotionally with wife, impatient with kids, isolated from friends.
- Daily Life: Avoid public places, always on edge, exhausted from poor sleep, using alcohol to cope.
NOW – current status:
“Still in treatment. Symptoms improved slightly with medication and therapy but far from resolved. PTSD is chronic and will require ongoing treatment. BH provider states I will likely need treatment for rest of my life. Medications: Sertraline 100mg, Prazosin 2mg, Trazodone 50mg. Weekly therapy for 5 years.”
💡 Key Takeaway from This Example: SSG Rodriguez provided EXTENSIVE detail – stressor events, specific symptoms, functional limitations, current status. This level of detail leads to accurate C&P exams and appropriate ratings.
His final conditions documented:
- PTSD (combat-related) – 15 symptoms detailed
- Depression (secondary to PTSD)
- TBI with persistent symptoms (migraines, memory, cognitive)
- Chronic back pain with sciatica
- Bilateral knee pain
- Right shoulder injury (post-surgery)
- Tinnitus (bilateral, constant)
- Hearing loss (bilateral)
- Sleep apnea (CPAP daily)
- Plantar fasciitis (bilateral)
- GERD
- Burn pit exposure (documented for future claims)
- Alcohol use disorder (secondary to PTSD)
Result: Comprehensive Documentation
SSG Rodriguez’s thorough SHA Part A led to:
- ✅ Appropriate C&P exam scheduling (7 separate exams)
- ✅ Well-documented conditions with service connection
- ✅ Environmental exposures recorded for future protection
- ✅ Strong foundation for successful VA claim
🚀 PART 8: What Happens After You Submit
Timeline, C&P exams, ratings, and final guidance
📅 Timeline: What to Expect
| Timeline | What Happens | What You Do |
|---|---|---|
| Week 0 | VA receives your SHA Part A, reviews conditions you’re claiming | Make copies of everything, save to secure USB drive |
| Weeks 1-4 | VA schedules C&P exams | Watch for letters/calls, mark calendar immediately |
| Weeks 2-8 | Attend all C&P exams | Use our C&P Exam Prep Guide, bring your SHA Part A copy |
| Weeks 8-20+ | VA reviews evidence and assigns ratings | Check claim status at VA.gov, be patient |
| Month 3-6+ | Receive decision letter with ratings | Review carefully, consider appeals if needed |
🎯 Top 10 C&P Exam Tips
1️⃣ Attend EVERY Exam
Missing exams = delays or denials
2️⃣ Bring Your SHA Part A
Reference it to stay consistent
3️⃣ Describe Your WORST Days
Not average days – how bad it gets
4️⃣ Be Specific
Don’t say “knee hurts” – detail pain level, limitations, frequency
5️⃣ Mention Frequency
Daily? Constant? Weekly flare-ups?
6️⃣ Discuss Impact
How it affects work, family, daily life
7️⃣ Be Honest About Mental Health
Don’t downplay depression, PTSD, suicidal thoughts
8️⃣ Bring a Written List
You’ll be nervous – write down all symptoms beforehand
9️⃣ Don’t “Push Through”
If it hurts to lift your arm – STOP and say it hurts
🔟 Ask for Clarification
Make sure examiner documents everything
📖 Deep Dive: Read our complete C&P Exam Preparation Guide before your exams. It covers exactly what to expect for each exam type (mental health, musculoskeletal, audiology, etc.).
💰 Understanding VA Ratings
VA rates conditions from 0% to 100% in 10% increments. Multiple conditions are combined using “VA math” (not simple addition).
Monthly Payment Examples (2024 rates, veteran without dependents):
- 10%: $165.92/month = $1,991/year
- 30%: $508.05/month = $6,097/year
- 50%: $1,041.82/month = $12,502/year
- 70%: $1,663.06/month = $19,957/year
- 100%: $3,737.85/month = $44,854/year
Use our VA Disability Calculator to estimate your combined rating.
📚 Additional Resources
🏠 VAMAX4U Home
Main website with guides, tools, and resources
❓ BDD FAQ
Common questions about BDD process
🧮 Calculator
🔍 Search Tool
Find condition info instantly
📖 Condition-Specific Appeal Guides
- PTSD Appeals Guide
- Back & Spine Appeals Guide
- Knee Appeals Guide
- Shoulder Appeals Guide
- TBI Appeals Guide
- Migraine Appeals Guide
- TDIU Appeals Guide
- Sciatica Appeals Guide
- Ankle Appeals Guide
- CUE Appeals Guide
💪 Final Words of Encouragement
You’ve Got This! 🎖️
You earned these benefits through your service.
You sacrificed. Your body and mind were affected. These aren’t handouts – you EARNED every penny through your service.
Be thorough. Be honest. Don’t minimize.
The VA can’t help you if they don’t know what’s wrong. Document everything. Use the WHEN-WHAT-HOW-NOW format. Get the benefits you deserve.
Thank you for your service. 🇺🇸
🎉 Guide Complete!
You now have everything you need to complete your SHA Part A Self-Assessment like a pro.
What’s next?
- ✅ Gather your documents
- ✅ Fill out your SHA Part A using this guide
- ✅ Make copies for your records
- ✅ Submit through your command or VSO
- ✅ Prepare for C&P exams with our prep guide